
November 26, 2020
Kevin Corbett MSc PGCE PhD is a retired nurse with over 37 years of
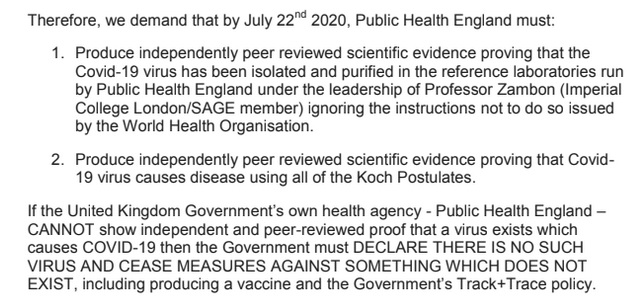
clinical nursing experience in England, a research consultant and health scientist. He has been a vocal critic of “COVID-19” hysteria and is a member of the StandUpX Science Committee that published an open letter dated June 22, 2020 to the British Prime Minister, Boris Johnson, demanding scientific proof of the alleged “COVID-19 virus”.
Below is a screenshot from the StandUpX open letter; the entire letter can be accessed from Dr. Corbett’s website, here.
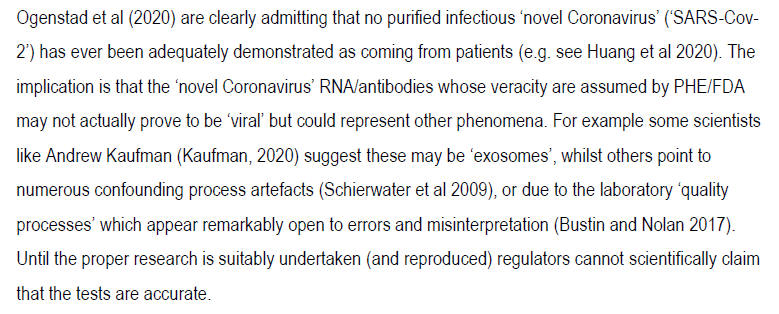
In April 2020 Dr. Corbett published a paper describing issues around the non-isolation of the theoretical SARS-COV-2 virus. Below is a screenshot from his paper entitled “Where is the evidence for the existence of the ‘novel coronavirus’, ‘SARS-CoV-2’, and the accuracy of the tests?”:
To this day, Public Health England (PHE) has still not produced the necessary evidence, as evidence by many FOIs responses from PHE; they can found here.
Dr. Corbett continues his efforts for “COVID-19” truth, very recently participating in an Irish “COVID-19” inquiry.
April 2020: Dr. Corbett contacted the Director of Reference Microbiology Services, Public Health England
Public Health England’s Deputy Director of National Infection Service and Director of Reference Microbiology Services is a British virologist and Imperial College London Professor, Maria Zambon FMedSci FRCPath.
Zambon is also a co-author on the infamous Corman-Drosten paper Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR that describes the development of “diagnostic methodology for use in public health laboratory settings without having virus material available“.
[Dr. Corbett co-authored the remarkable Corman-Drosten Review Report that identified 10 major scientific flaws at the molecular and methodological level for the diagnostic methodology developed by Zambon, Corman, Drosten et al.]

In April and May of 2020, Dr. Corbett contacted Professor Zambon in her capacity as Director of Reference Microbiology Services with questions regarding the “COVID-19” tests used in England and Wales, and the UK in general.
Dr. Corbett has kindly agreed to make the resulting communications public, in the public interest. His questions and the responses he received from Public Health England (PHE) are provided below in downloadable pdfs.
The commentary that follows is my own; Dr. Corbett bears no responsibility for any of it.
Please keep in mind when reviewing these communications that the tests in questions are for a purely theoretical virus. Wild speculation and fraudulent claims are the basis of worldwide belief in “COVID-19”, not the scientific method. If that sounds like an outrageous claim, I recommend familiarizing yourself with the information available here: “So What The Hell Is Going On?“, and dozens of additional Freedom of Information responses from around the world that are available on this page.
Some Background
Before looking at the communications between Dr. Corbett and Professor Zambon, it’s interesting to note a statement issued by Public Health England, last updated June 2, 2020, entitled “Position statement regarding COVID-19 tests evaluated by PHE“. A screenshot is shown below and it’s available online here:
https://www.gov.uk/government/publications/position-statement-regarding-covid-19-tests-evaluated-by-phe/position-statement-regarding-covid-19-tests-evaluated-by-phe
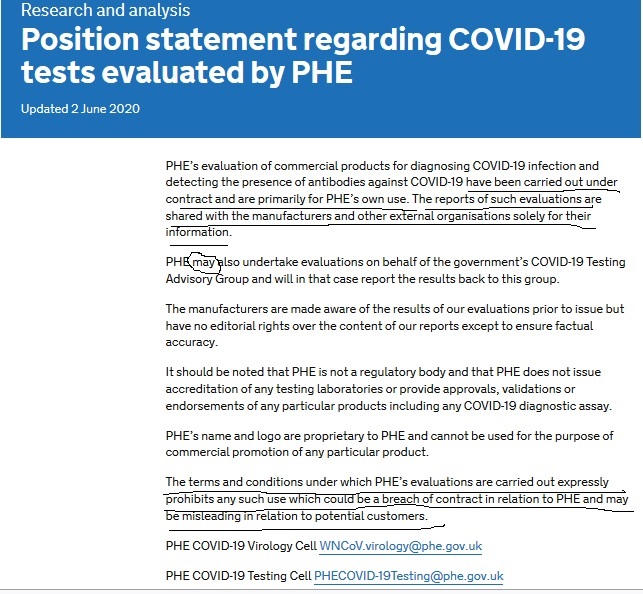
So Public Health England is under contract with “COVID-19” commercial test manufacturers to evaluate their tests? Or Public Health England contracts with someone else to evaluate those commercial tests? Either way, I’m getting the distinct impression that the terms and conditions of Public Health England’s contracts are such that the interests of the manufacturers are prioritized over the interests of the public.
And it seems that even though Public Health England evaluates commercial “COVID-19” tests, they don’t necessarily consider the tests even remotely legitimate and certainly don’t want to be held responsible for them. Interesting.
Now for the communications between Dr. Corbett and Professor Zambon, Director of Reference Microbiology Services at Public Health England.
Public Health England admits using fake “SARS-COV-2” material to evaluate “COVID-19” tests and that isolated virus is not the gold standard
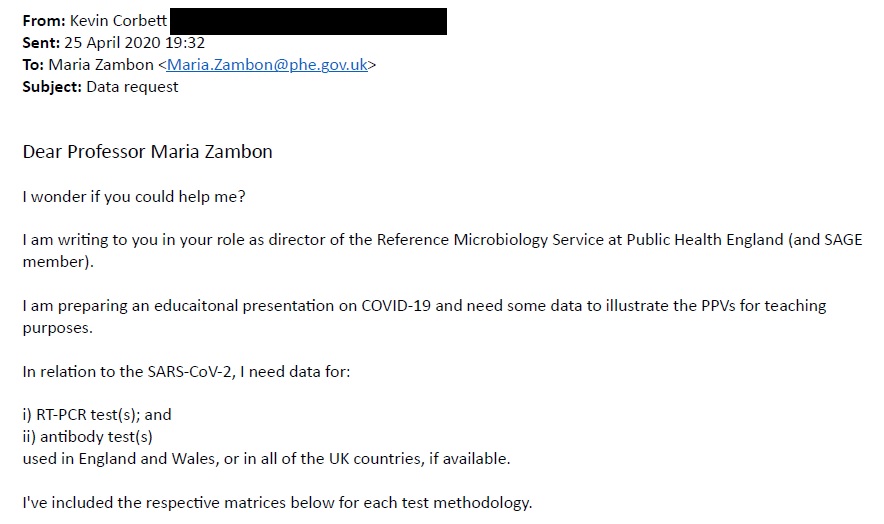
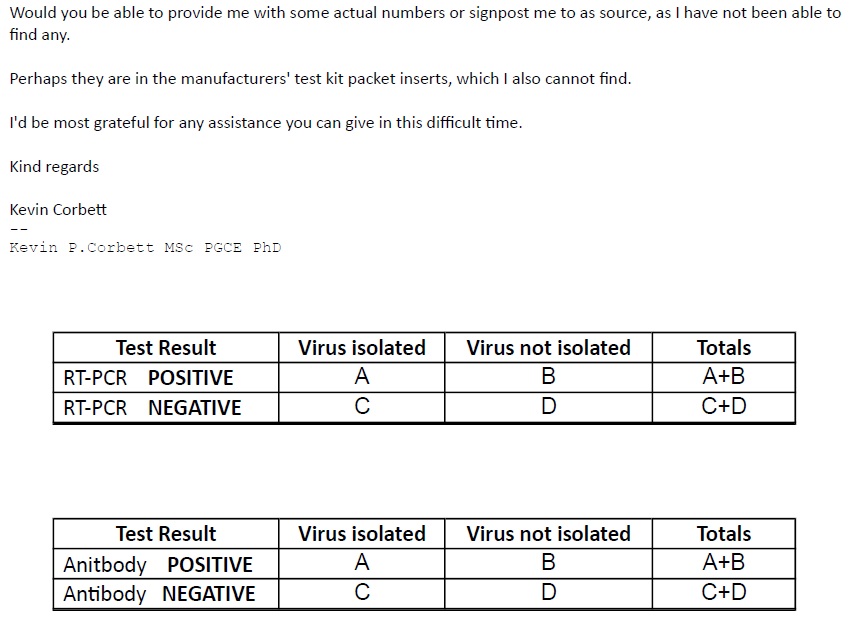
Dr. Corbett’s initial email (April 25 2020) to Professor Zambon is shown below. He requested from Professor Zambon data required for calculation of the positive predictive value (PPV) of the “COVID-19” PCR and antibody tests.
Public Health England’s email response to Dr. Corbett is shown below. It was sent by an anonymous man or woman at the “PHE COVID-19 Virology Cell” with Professor Zambon cc’d.
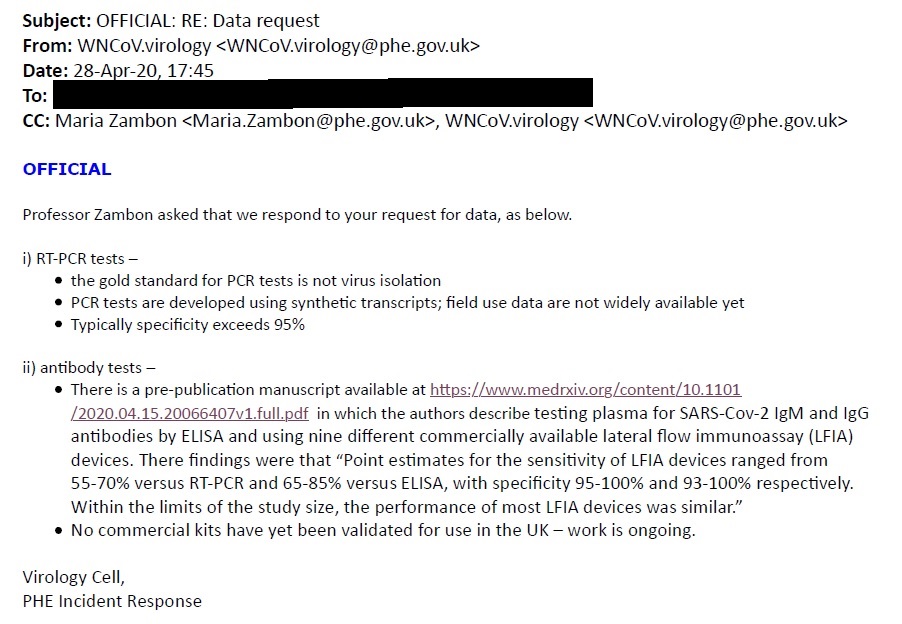
The PHE COVID-19 Virology Cell admitted flat out that “the gold standard for PCR tests is not virus isolation” and “PCR tests are developed using synthetic transcripts; field use data are not widely available yet“.
This corresponds to admissions in the Corman-Drosten-Zambon paper mentioned earlier. The researchers did not have any samples of the alleged virus, and so they assessed the accuracy of their PCR testing methodology using:
1) the genetic soup referred to as “cell culture supernatant” (alleged but never proven to contain the 2003 SARS-COV), and
2) synthetic “SARS-COV-2” genetic material… since no actual SARS-COV-2 virus was available; see:
https://www.eurosurveillance.org/content/10.2807/1560-7917.ES.2020.25.3.2000045#html_fulltext
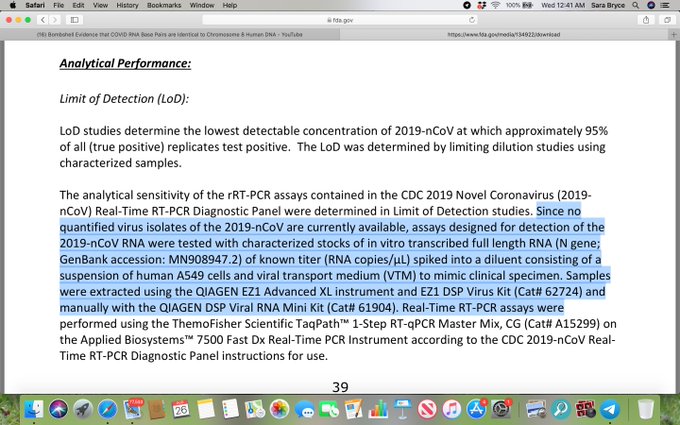
PHE’s response also parallels the admission made on page 39 of the U.S. Centres for Disease Control’s “2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel” (revision 5, effective 07/13/2020): “Since no quantified virus isolates of the 2019-nCoV are currently available, assays designed for detection of the 2019-nCoV RNA were tested with characterized stocks of in vitro transcribed full length RNA…”
[Note that 2019-nCoV was the original name given to the alleged “SARS-COV-2”.]
https://www.fda.gov/media/134922/download.
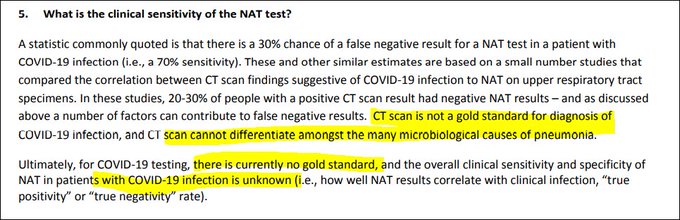
The response from PHE also fits with a statement published by the British Columbia (Canada) Centre for Disease Control | BC Ministry of Health in a document entitled Interpreting the results of Nucleic Acid Amplification testing (NAT; or PCR tests) for COVID-19 in the Respiratory Tract dated April 30, 2020. In the midst of contradictions and misinformation, the BC CDC disclosed that: “for COVID-19 testing, there is currently no gold standard….”
http://www.bccdc.ca/Health-Professionals-Site/Documents/COVID19_InterpretingTesting_Results_NAT_PCR.pdf.
Up to 5% of all “COVID-19” PCR tests could yield a false positive?
The PHE COVID-19 Virology Cell went on to claim that for the RT-PCR tests “Typically specificity exceeds 95%“.
Specificity is the proportion/percentage of those who in fact do not have the thing being tested for, that accurately receive a negative test result. (And 100% – specificity is the percentage of those without the thing tested for who inaccurately test positive.) In the tables at the end of Dr. Corbett’s email specificity = D / (B+D).
In the case of a purely theoretic virus like “SARS-COV-2”, B+D represents everyone who is tested, and specificity is the proportion/percentage of all tests that are negative.
Thus it seems that a straightforward interpretation of the PHE COVID-19 Virology Cell’s response is that anywhere up to 5% of all “COVID-19” PCR tests could yield a false positive. (Keep that in mind when researching Operation Moonshot, the UK government’s proposed “COVID-19” mass testing scheme.)
[Regardless of PHE’s estimates, one thing is certain: if an alleged virus is in fact purely theoretical, all positive test results, 100% of them, are false positives.]
The PHE COVID-19 Virology Cell then went on to cite a pre-publication manuscript providing estimates of the sensitivity and specificity of “COVID-19” antibody tests.
Sensitivity is the proportion/percentage of those who in fact do have the thing being tested for, that receive a positive test result. In the tables at the end of Dr. Corbett’s email sensitivity = A / (A+C).
In the case of a purely theoretical virus like “SARS-COV-2”, A and C are both zero and sensitivity is undefined. Thus estimates of sensitivity for any “COVID-19” tests are nonsensical.
Having as of today, November 26, 2020, collected >40 letters from >34 institutions around the world (obtained by myself and colleagues in various countries) yielding in total zero evidence for the existence of “SARS-COV-2”, I personally do not have any interest or energy left for discussions of sensitivity or “COVID-19” antibody tests at all. [October 22, 2021 update: we now have responses from 121 institutions in at least 24 countries.] But for those who do, here is the pre-publication manuscript cited by the anonymous source at the PHE COVID-19 Virology Cell:
“Evaluation of antibody testing forSARS-CoV-2 using ELISA and lateral flow immunoassays
AUTHORSHIP: National COVID Testing Scientific Advisory Panel… CORRESPONDING AUTHOR: Prof Derrick CrookDepartment of Microbiology, John Radcliffe Hospital, Oxford,OX3 9DU, United Kingdom”: https://www.medrxiv.org/content/10.1101/2020.04.15.20066407v1.full.pdf
Both the April query from Dr. Corbett and the anonymous response from the PHE COVID-19 Virology Cell are available for download in a pdf here: https://www.fluoridefreepeel.ca/wp-content/uploads/2020/11/Public-Health-England-response-re-COVID19-test-PPVs-April-2020-scrubbed.pdf.
Dr. Corbett followed up with 12 additional questions for Zambon.
Once again, an anonymous man or woman responded from the “Public Health England COVID-19 Virology Cell” on behalf of Maria Zambon.
The 12 questions and answers are here:
https://www.fluoridefreepeel.ca/wp-content/uploads/2021/02/May-2020-Q-and-A-emails-Dr.-Corbett-and-PHE-plus-attachment.pdf
Dr. Corbett’s notes re PHE’s answers:
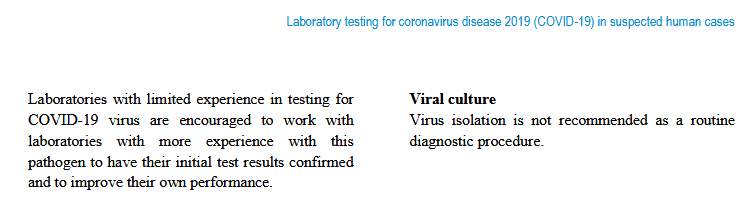
- ‘Viral isolation’ not advised in accordance with instructions from the World Health Organisation, para 6, interim guidance, 2 March 2020: ‘Laboratory testing for coronavirus disease 2019 (COVID-19) in suspected human cases’. This showed to me that the UK National Health Service is under the scientific guidance [?jurisdiction] of the World Health Organisation.
- [competing narratives: isolation not advised, isolation impossible, isolation done many times]
- Re gold standard for PCR test: PHE referred me to the Corman et al (2020) paper that implies the gold standard is a repeated PCR: using the same test methodology as its own reference standard without viral isolation.
- My other questions weren’t clearly answered; and I was referred back to the attached Corman et al (2020), and to other government publications, which I think are still accessible on the links PHE supplied.
See page 4 of the WHO’s Interim Guidance document dated March 2, 2020 “Laboratory testing for coronavirus disease 2019 (COVID-19) in suspected human cases” kindly provided by Dr. Corbett and preserved here: https://www.fluoridefreepeel.ca/wp-content/uploads/2020/11/WHO-COVID-19-laboratory-2020.4-eng.pdf
Apparently public health officials around the world decided to go a step further by requiring no isolation/purification of any “SARS-COV-2” by anyone on the planet, ever, and thus declare a “pandemic” based on wild industry-serving assumptions and illogic.
Find Dr. Corbett on Twitter at @KPCResearch.
StandUpX has a petition entitled “If there’s no proof the virus exists end all Lockdowns/Masks/Trax/Vax actions“. If you can tell the difference between isolating something and mixing things together, please consider signing it, here:
https://www.gopetition.com/petitions/if-theres-no-proof-the-virus-exists-end-all-lockdownsmaskstraxvax-actions-2.html