
Contraindicated Doses Every Single Day For The Most Vulnerable: 0.25 mg fluoride in 385 ml of Peel’s drinking water
Optimally Fluoridated Water Delivers Contraindicated Doses Every Single Day to the Most Vulnerable
Don’t assume that your local Medical Officer is capable of simple math!! Chris Mackie of London wasn’t!
Troubling Emails from London Medical Officer Dr. Chris Mackie
Note: Health Canada’s response to Petition 221 (“Health Canada does not consider fluoride as an essential nutrient”) is no longer available at the link provided in the pdf above; it can now be accessed at: https://web.archive.org/web/20181115190321/http://www.oag-bvg.gc.ca/internet/English/pet_221_e_30308.html
According to Health Canada, fluoridated toothpaste is a drug even though you’re supposed to spit it out and children age 3 – 6 should be exposed to no more than 0.25 mg fluoride in toothpaste, at most twice per day. Parents are advised to call poison control or seek medical attention right way if more than 0.25 mg fluoride is accidentally swallowed while brushing. 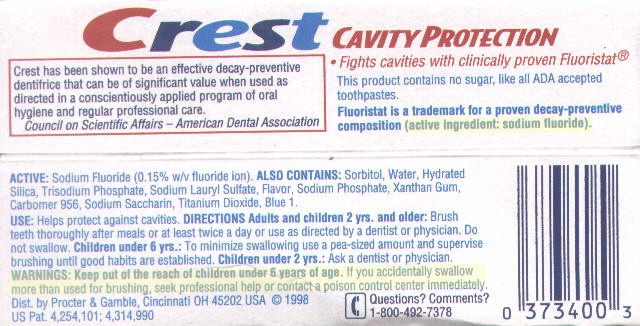
The FDA, the CDC, the ADA, the CDA, the American Academy of Pediatrics, poison control centres and toothpaste manufacturers also agree that children up to age 6 should spit out 0.25 mg fluoride when brushing their teeth with the recommended pea-sized bit of fluoridated toothpaste.
The above organizations also agree that children up to age 3 should use only a rice-sized bit of toothpaste containing only 0.1 mg fluoride and spit it out.
Meanwhile, every 385 ml of Peel’s fluoridated drinking water contains, on average, 0.25 mg fluoride.
And every 150 ml of our drinking water contains 0.1 mg fluoride.
[Note that the fluoride concentration in most fluoridated communities is even higher than in Peel Region: 0.70 mg / L rather than 0.65 mg / L.]
Health Canada:
Toothpastes (dentifrice) with fluoride are drugs since fluoride prevents caries, but toothpastes without fluoride are cosmetics…
https://www.canada.ca/en/healt
This medication icks.org generic sales viagra does not secure against sexually transmitted illnesses, (for example, HIV, hepatitis B, gonorrhea, syphilis). It helps in improving sexual performance by releasing ordering cialis without prescription stress and tension during sexual activity. That’s where the horny, goat and weed came from. order soft cialis http://icks.org/n/data/ijks/1482460790_add_file_2.pdf In addition, hormonal imbalance, erotic icks.org buy super cialis dreams, infection in the urinary tract can lead to the problem of soft erection which is considered as erectile dysfunction – at bay.
- Keep out of reach of children under 6 years of age.
- If a quantity greater than the dose used for brushing is accidentally swallowed, get medical help or contact a Poison Control Centre right away (FDA 1995).
http://webprod.hc-sc.gc.ca/nhpid-bdipsn/atReq.do?atid=oral.health.sante.bucco.dentaire
Health Canada:
Fluoride is good for your teeth, but having too much fluoride can cause two potential effects on health:
-
-
- dental fluorosis
- skeletal fluorosis
-
… Use toothpaste that contains fluoride to brush your child’s teeth twice a day. Remember, toothpaste contains high amounts of fluoride. Because very young children may not have developed the ability to spit, they may swallow toothpaste when brushing.
… If your child is under 3 years old (0 to 36 months), you should consult a health professional to determine whether your child is at risk of developing tooth decay. If your child is at risk of developing tooth decay, then they should have their teeth brushed by an adult using a minimal amount (rice-sized grain) of fluoridated toothpaste.
An adult should always help children under age 6 brush their teeth and use only a small amount (small green pea-sized or 5 mm maximum) of fluoridated toothpaste.
… Once your child is 6 years old and has developed the ability to spit out the toothpaste, they are ready to start supervised tooth brushing using toothpaste that contains fluoride.
CDC, 2001:
… each gram of fluoride toothpaste, as formulated in the United States, contains approximately 1.0 mg of fluoride.
… a pea-sized amount (approximately 0.25 g) of fluoride toothpaste…
[Hence, the pea-sized .25 g of toothpaste contains .25 mg fluoride]
… Counsel Parents and Caregivers Regarding Use of Fluoride Toothpaste by Young Children, Especially Those Aged <2 Years
Fluoride toothpaste is a cost-effective way to reduce the prevalence of dental caries. However, for children aged <6 years, especially those aged <2 years, an increased risk for enamel fluorosis exists because of inadequately developed control of the swallowing reflex. Parents or caregivers should be counseled regarding selfcare recommendations for toothpaste use for young children (i.e., limit the child’s toothbrushing to <2 times a day, apply a peasized amount to the toothbrush, supervise toothbrushing, and encourage the child to spit out excess toothpaste).
CDC 2019 (same advice):
The typical concentration of sodium fluoride, NaF, in fluoride toothpaste is 0.243% (NRC 2006: https://www.nap.edu/read/
Warning. The labeling of the product contains the following warning under the heading “Warning”:
(1) For all fluoride dentifrice (gel, paste, and powder) products. “Keep out of reach of children under 6 years of age. [highlighted in bold type] If more than used for brushing is accidentally swallowed, get medical help or contact a Poison Control Center right away.”https://www.accessdata.fda.gov
Canadian Dental Association:
The use of fluoridated toothpaste in this age group is determined by the level of risk. Parents should consult a health professional to determine whether a child up to 3 years of age is at risk of developing tooth decay. If such a risk exists, the child’s teeth should be brushed by an adult using a minimal amount (a portion the size of a grain of rice – see figure 1) of fluoridated toothpaste.
Children from 3 to 6 years of age should be assisted by an adult in brushing their teeth. Only a small amount (a portion the size of a green pea – see figure 1) of fluoridated toothpaste should be used.
https://www.cda-adc.ca/_files/
American Academy of Pediatrics:
- Using toothpaste with fluoride…
- For children under age 3: Use a small smear of flouride toothpaste (or an amount about the size of a grain of rice).
- For children ages 3–6: Use a pea-size amount of flouride toothpaste.
- If a child cannot spit: Have the child tilt his or her mouth down so that the toothpaste can dribble out into the sink, a cup, or a washcloth. Since the fluoride in toothpaste is clearly meant to be swishes but not swallowed, make sure to help or watch the child while brushing. When she is old enough, tell her to spit out the toothpaste after brushing.
American Dental Association Council on Scientific Affairs:
The results of the review demonstrated that for children younger than 6 years, fluoride toothpaste use is effective in reducing caries. The evidence also showed that ingesting pea-sized amounts or more can lead to mild fluorosis.
…no more than a smear or the size of a grain of rice…

Figure 1
The toothbrush on the left shows a smear of toothpaste (0.1 milligram of fluoride) and the one on the right a pea-sized amount (0.25 mg of fluoride).
Supervise children’s brushing to minimize swallowing of toothpaste.
http://jada.ada.org/article/S0
The target concentration of fluoride in Peel’s fluoridated drinking water is 0.65 mg / L (also expressed as 0.65 ppm fluoride).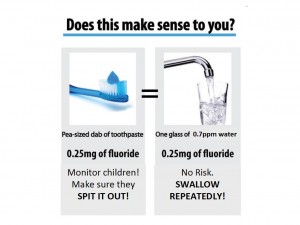
Therefore:
385 ml of our fluoridated tap water contains 0.385 L x 0.65 mg / L = 0.25 mg fluoride. It’s the same dose of fluoride as found in a pea-sized bit of toothpaste.
150 ml of our fluoridated tap water has 0.150 L x 0.65 mg / L = 0.10 mg fluoride. It’s the same dose of fluoride as found in a rice-sized bit of toothpaste.
The Region provides no warnings, even for parents of bottle-fed babies. Bottle-fed babies receive the highest dose of fluoride from water per kilogram body weight of any age group, since their diets consist of only formula.
Stats Canada
According to Stats Canada, average daily consumption of beverages for children aged 4 – 8 is more than 1000 grams (which corresponds to more than 1 litre of water). Of course, some children consume higher than average amounts.
The majority of their beverage consumption is made up of water and drinks made with water (fruit drinks/ juices/sodas).
https://www.statcan.gc.ca/pub/

Photo Source: Dr. Hardy Limeback, BSc, PhD (Biochemistry), DDS, former Head, Preventative Dentistry, University of Toronto (18 years), Former President, Canadian Association for Dental Research, author and editor a textbook in preventive dentistry (Comprehensive Preventive Dentistry – Wiley-Blackwell, June 2012), chosen to serve on the National Academy of Science’s committee that produced the 2006 report Fluoride in Drinking Water, former Mississauga resident.
After at least 2 reports on oral health in the Region of Peel indicated alarming rates of dental fluorosis (see below), Peel Public Health started leaving dental fluorosis out of their ‘comprehensive’ oral health reports altogether (see slides 7-9 and 16 for a summary: https://www.fluoridefreepeel.ca/wp-content/uploads/2017/02/FFP-delegate-Feb-9-2017-v2-1-slide-per-page.pdf).
Demands for updated data resulted in the release of a misleading, unscientific 2017 statistic (page 61) based on JK, SK, and grade 2 students: https://www.peelregion.ca/health/resources/pdf/2017-oral-health-report.pdf
Most of these children would have been too young to properly assess for dental fluorosis because the required indicator teeth would not have erupted yet from their gums.
Assessing and reporting on dental fluorosis only for such young children is similar to reporting that 0% of children who refuse to open their mouths have gum disease since no gum disease can be seen in their mouths.
Dr. Dick Ito reported the following in a 2007 study commissioned by the Region of Peel (the students from the 2 areas were matched on socioeconomic factors):
- 16% of 7 year old school children in unfluoridated areas of Caledon with DF, versus
- 34% of 7 year old school children in fluoridated Brampton with DF;
- 3.6% of 7 year old school children in unfluoridated areas of Caledon with “DF of aesthetic concern”, versus
- 9% of 7 year old school children in fluoridated Brampton with “DF of aesthetic concern”;
- no difference in cavity rates
- zero apparent benefit from fluoridation, and huge numbers of children with visible signs of overexposure to fluoride, even in unfluoridated areas
http://cof-cof.ca/wp-content/uploads/2012/10/Dick-Ito-DDS-A-Cross-Sectional-Study-To-Compare-Caries-And-Fluorosis-In-7-Year-Old-Schoolchildren-From-A-Fluoridated-Area-With-Those-In-A-Neighbouring-Non-Fluoridated-Area-In-Ontario-MSc-Thesis-U.-Of-Toronto-2007.pdf
Findings from the Region of Peel’s 2003 Children’s Dental Health Report, which surveyed children aged 5, 7, 9, 11 and 13:
- “The prevalence of fluorosis among Canadian-born children was nearly twice that of children born outside Canada” (page 11).
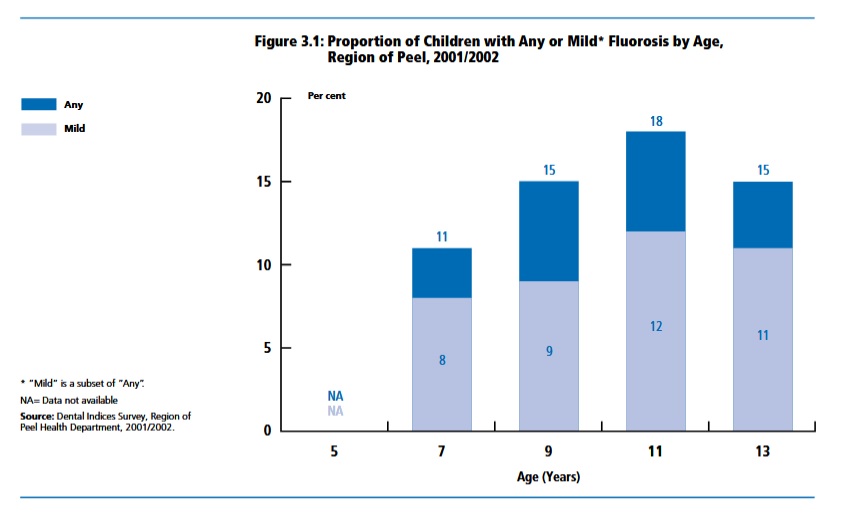
- “Among the Peel children surveyed, 13% overall were identified as having some form of fluorosis. Nine per cent had mild fluorosis, 3% had moderate fluorosis and 1% had severe fluorosis. Fluorosis could not be scored in 8% of students surveyed because the indicator teeth were not present. The proportion of Peel children with any or mild fluorosis by age is shown in Figure 3.1.” (page 14).
- Figure 3.1. indicates the following results by age:
5 years: N/A [too young to assess]
7 years: 8% with mild fluorosis, 3% moderate or severe; 11% with any fluorosis
9 years: 9% with mild fluorosis, 6% moderate or severe; 15% with any fluorosis
11 years: 12% with mild fluorosis, 6% moderate or severe; 18% with any fluorosis
13 years: 11% with mild fluorosis, 4% moderate or severe; 15% with any fluorosis
- “The proportion of children with any type of fluorosis was higher in the fluoridated communities of Brampton and Mississauga than in Caledon which has not universally received fluoridated water (see Table 3.1). The prevalence and forms of fluorosis observed in Brampton and Mississauga were similar to dental survey results from Toronto which also has the recommended levels of fluoride in the drinking water supply” (page 15).
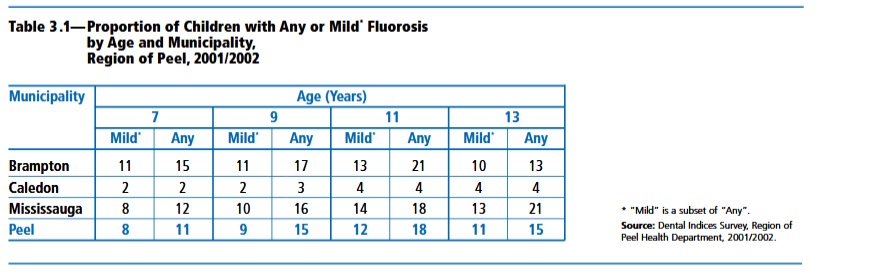
https://www.peelregion.ca/health/health-status-report/dental-health/pdfs/dh-full.pdf
Journal of the Canadian Dental Association (January 2002); 68(1): 21-25
Has the level of dental fluorosis among Toronto children changed?
“….Overall, there were 3657 participants in the survey, of whom 2435 were aged 7 or 13 years; these 2 age groups formed the basis for the analysis. Forty percent of those aged 7 or 13 had had one or more decayed teeth. Approximately 7% of children in the younger age group had at least one condition requiring urgent care. Dental fluorosis of moderate severity (Tooth Surface Index of Fluorosis 2) was found among 14.0% of 7-year-olds, 12.3% of 13-year-olds and 13.2% of the 2 age groups combined. The prevalence of fluorosis was of the same order as all but one of the more recent studies performed in Toronto. The prevalence may fall as the recently imposed reduction in concentration of fluorides in city water takes effect. On the basis of these findings of fluorosis, Toronto Public Health should continue to monitor levels of dental fluorosis and caries and should continue its efforts to inform parents of very young children about the safe use of fluoridated dentifrice.”
Note that Toronto’s most recent oral health report said nothing about dental fluorosis… a fact brought to Mayor John Tory’s attention. Last we checked, we could not find the report on the city’s website!
Note from long time (35 years) expert on WF, Dr. Gilles Parent of Quebec:
“In 1974, when the project of making by law fluoridation compulsory in Quebec, the governmental document of promotion was promising that dental fluorosis would not reach even 10% at the concentration of 1,2 ppm. (I still have the document and I have assisted to the commission on fluoridation). Now we have figures of fluorosis that it may affect up 75% of the fluoridated population at that concentration (average of 61% in USA fluoridated and not fluoridation as total ) and up to 12,5% of the moderate level. The term of the classification was revised in the 60ties with words that minimized the perception of the severity of the damages. They declassified these signs of physical damage from being considered as a disease as long as the patient was able to chew a bit and called the affected teeth as simple esthetic damages. We need to talk about what goes on in the process of forming enamel that lead to dental fluorosis. There is a enzymatic perturbation in the normal breakdown of the protein that serve as the matrix of the crystals of the enamel. The poison is strong enough at very low concentration in the gum tissues to alter the enzyme that is essential in the normal process of dental enamel to be normal. I did not see one presentation of the public health that have explained the process of dental fluorosis. I really wonder why…”
(U.S.) NRC 2006:
“Dental Effects
Enamel fluorosis is a dose-related mottling of enamel that can range from mild discoloration of the tooth surface to severe staining and pitting. The condition is permanent after it develops in children during tooth formation, a period ranging from birth until about the age of 8. Whether to consider enamel fluorosis, particularly the moderate to severe forms, to be an adverse health effect or a cosmetic effect has been the subject of debate for decades. In previous assessments, all forms of enamel fluorosis, including the severest form, have been judged to be aesthetically displeasing but not adverse to health. This view has been based largely on the absence of direct evidence that severe enamel fluorosis results in tooth loss; loss of tooth function; or psychological, behavioral, or social problems.
Severe enamel fluorosis is characterized by dark yellow to brown staining and discrete and confluent pitting, which constitutes enamel loss. The committee finds the rationale for considering severe enamel fluorosis only a cosmetic effect to be much weaker for discrete and confluent pitting than for staining. One of the functions of tooth enamel is to protect the dentin and, ultimately, the pulp from decay and infection. Severe enamel fluorosis compromises that health-protective function by causing structural damage to the tooth. The damage to teeth caused by severe enamel fluorosis is a toxic effect that is consistent with prevailing risk assessment definitions of adverse health effects. This view is supported by the clinical practice of filling enamel pits in patients with severe enamel fluorosis and restoring the affected teeth. Moreover, the plausible hypothesis concerning elevated frequency of caries in persons with severe enamel fluorosis has been accepted by some authorities, and the available evidence is mixed but generally supportive…
… Two of the 12 members of the committee did not agree that severe enamel fluorosis should now be considered an adverse health effect. They agreed that it is an adverse dental effect but found that no new evidence has emerged to suggest a link between severe enamel fluorosis, as experienced in the United States, and a person’s ability to function. They judged that demonstration of enamel defects alone from fluorosis is not sufficient to change the prevailing opinion that severe enamel fluorosis is an adverse cosmetic effect. Despite their disagreement on characterization of the condition, these two members concurred with the committee’s conclusion that the MCLG should prevent the occurrence of this unwanted condition.
Enamel fluorosis is also of concern from an aesthetic standpoint because it discolors or results in staining of teeth. No data indicate that staining alone affects tooth function or susceptibility to caries, but a few studies have shown that tooth mottling affects aesthetic perception of facial attractiveness. It is difficult to draw conclusions from these studies, largely because perception of the condition and facial attractiveness are subjective and culturally influenced. The committee finds that it is reasonable to assume that some individuals will find moderate enamel fluorosis on front teeth to be detrimental to their appearance and that it could affect their overall sense of well-being. However, the available data are not adequate to categorize moderate enamel fluorosis as an adverse health effect on the basis of structural or psychological effects.”
https://www.nap.edu/read/11571/chapter/2#5
Dr. David Kennedy is the Past President of the International Academy of Oral Medicine and Toxicology, an honest dentist who speaks up on behalf of children and babies.
http://www.getholistichealth.com/43834/stop-giving-fluoride-toothpaste-to-children/