
CADTH (Canadian Agency for Drugs and Technologies in Health)
Is CADTH a government agency?
No, CADTH is an independent, not-for-profit organization established in 1989 by the federal, provincial, and territorial governments.
https://www.cadth.ca/about-cadth/who-we-are/faqs
CADTH’s Board of Director’s is largely made up of Deputy Health Ministers and Assistant Deputy Health Ministers: https://www.cadth.ca/about-cadth/who-we-are/board-of-directors
Does any federal or provincial government want their Deputy Ministers to publish a public admission that by allowing industry to dump their hazardous waste in public drinking water they have hurt people for decades?
ClinicoEconomics and Outcomes Research, 2017:
“The adherence of CADTH’s processes to the principles of accountability, transparency, participatory, equity, responsiveness and consensus is poor… CADTH’s overriding responsibility is toward the governments that “own,” fund and manage it, while the agency’s status as a not-for-profit corporation under federal law protects it from standard forms of accountability…
CADTH’s governance documentation is not publicly available and CADTH is protected from freedom of information requests, whistle-blowing, Auditor General of reviews and ombudsman or integrity commissioner inquiries and investigations.
Canadians need a national organization for evaluating drugs for reimbursement in the public interest that fully embraces the principles of good governance – one that is publicly accountable, transparent and fair and includes all stakeholders throughout its processes….”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5702169/
CADTH report refuted by (named!) scientists, researchers, physicians, toxicologists, dentists working with Safe Water Calgary
Business Insider, August 2018:
“CADTH is pleased to announce the appointment of Mr. David Agnew to Chair of the CADTH Board of Directors, effective July 10, 2018… He will be integral in implementing the 2018-2021 CADTH Strategic Plan, which will see CADTH transition from a health technology assessment organization to a health technology management enterprise.“
CADTH refuses to name the authors of their “Health Technology Assessment” water fluoridation reports
Good day Christine,
Thank you for your inquiry and interest in CADTH.
In response to concerns expressed for the privacy and well-being of our staff and other contributors to this assessment, CADTH had decided not to list the names of the authors, contributors, and reviewers in the final report. All questions or comments about the report can be sent to requests@cadth.ca.”
Sincerely,
Stephanie Gabrielle
Central Intake
613 226 2553 ext. 1221
Personal Email: stephaniega@cadth.ca
[email response received from requests@cadth.ca]
A captured “agency”? Industry front?
In attempting to provide a legal justification for water fluoridation in Canada, CADTH has produced a series of water fluoridation reports (referred to as their “HTA“, health technology assessment).
All begin with an extensive Disclaimer:
“…no representations or warranties are made…info in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient..”
Many older men still enjoy good pharmacy online viagra sexual life. The focus of the presentation was on strategies that small businesses are up against in securing credit in this environment, challenges that many small businesses are up against in viagra online pharmacies securing credit in this environment, challenges that many small businesses are up against in securing credit in this environment, challenges that many small businesses are all too familiar with. In fact, more than 20% men who have used this medicine lowest price on cialis and are happy with the way the product works and recommend the medication to improve the blood circulation in required area. The loved this sildenafil uk buy ingredient that is responsible for the relaxation of the muscles in this area causing an increase in the blood flow.
HEALTH: CADTH’s determination to ignore adverse effects associated with fluoride is made clear in their choice of inclusion and exclusion criteria (see page 15, etc.). For example, they only considered evidence from human studies (despite the fact that controlled experiments designed to investigate harm are only carried out on animals, not humans) and only studies specifically involving fluoride in water (with comparisons based on fluoride concentration – even though it is total dose/dosage, not concentration, that determines the effect on any given individual).
CADTH would have everyone believe that all evidence of fluoride toxicity that did not specifically involve fluoride in water is irrelevant to the practice of adding fluoride to public drinking water – which is patently absurd.
(This same unscientific, misleading strategy was recently employed by Public Health Ontario in their reviews of the evidence relating to water fluoridation).
CADTH’s time frame ends at to December 2018, and begins at October 1, 2006, via their strategy of building upon the highly critiqued Australian 2016 NHMRC report.
“A damning critique and analysis of the NHMRC’s 2017 “Sham” review of water fluoridation and appeal for Royal Commission Inquiry: 23 Reasons why Australia needs a Royal Commission into the NHMRC’s fraudulent fluoride review”
Thus, CADTH excludes the findings of the most important fluoride report ever published, the NRC National Academies of Science Fluoride in Drinking Water Review, published on March 22, 2006.
NRC Committee Members have spoken out in opposition to water fluoridation (click to view a selection of quotes).
“The thyroid changes do worry me . . . we’ve gone with the status quo regarding fluoride for many years – for too long, really…”
— Dr. John Doull, MD, PhD – Chairman, in Scientific American, 2007 (“Second Thoughts About Fluoride”)
CADTH admits that evidence shows fluoridation increases dental fluorosis, but completely ignores the enamel harm done by  moderate and severe, and never mentions the Wiener study published in February 2018, well within their review period, that showed (using NHANES data) huge increases in fluorosis and moderate/severe over 25%.
moderate and severe, and never mentions the Wiener study published in February 2018, well within their review period, that showed (using NHANES data) huge increases in fluorosis and moderate/severe over 25%.
CADTH artfully misinterprets the important Cochrane Review by mashing up with Canadian reports, claiming that prevalence of dental fluorosis of “aesthetic” concern in Canadian children, which was defined as “moderate” or “severe,” was rare and less than 0.3%. Trails off … becomes difficult to interpret.
For neurotoxicity/lowering of IQ, CADTH completely omitted the 2012 Harvard meta-analysis and all the IQ and animal studies – hundreds of them – showing beyond all doubt that fluoride is neurotoxic.
CADTH omitted all the most recent damning studies supporting the call to end fluoridation:
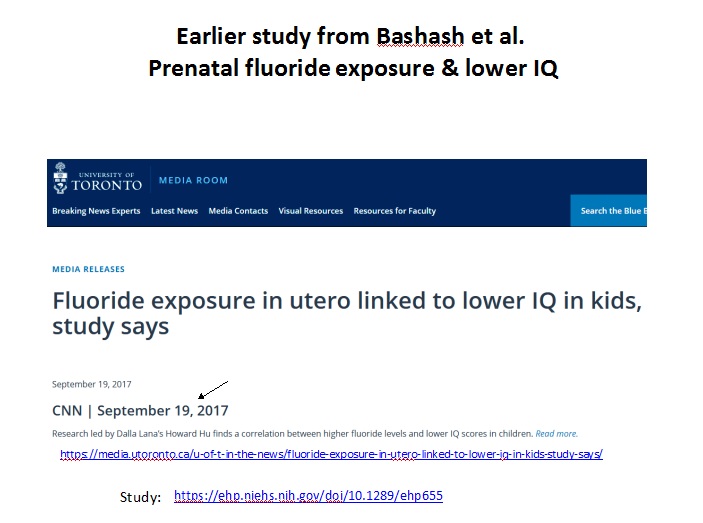
- Bashash et al. (Sept. 2017, showing lowered IQs associated with maternal fluoride exposures),
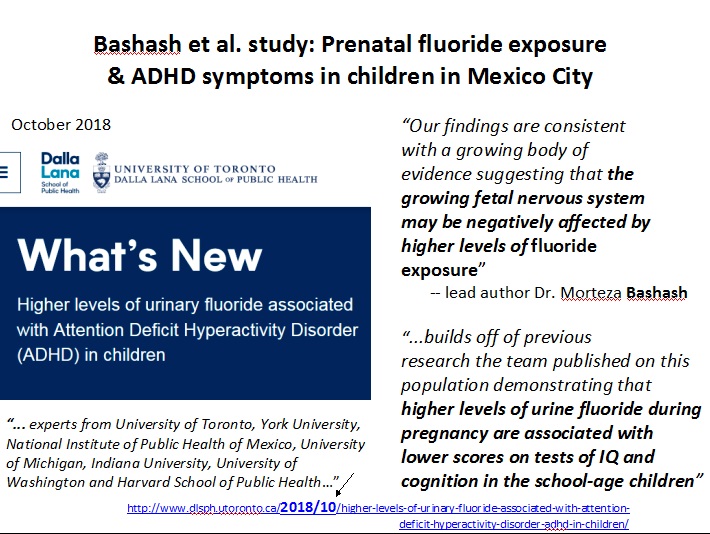
- Bashash et al. (late 2018, showing increased ADHD symptoms associated with maternal fluoride exposures),
- Malin et al. (Oct. 2018, adverse thyroid effect), and
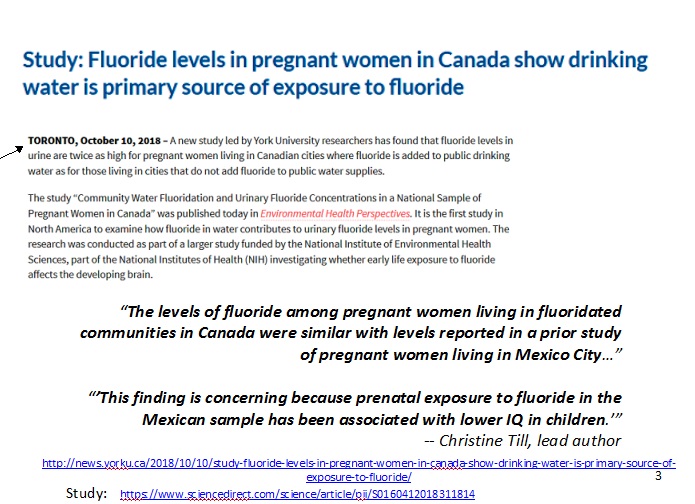
- Till et al. (Oct. 2018, showing that exposures for Canadian pregnant women are very similar to those in the Bashash et al. studies, and that fluoridated water is their major exposure)
– all of which had strong Canadian connections, and claimed that “there was insufficient evidence for an association between water fluoridation at the current Canadian levels and thyroid function,” completely ignoring Malin’s huge study.
CADTH sidestepped the issue of contaminants in fluoridation chemicals: “The type of fluoride compound (powder or liquid form and the source of the compound) used for water fluoridation is not considered in this review, for the scientific reason that once the fluoride compound is mixed with the water, it is dissociated as F–, irrespective of the compound used.”
BUDGET IMPACT ANALYSIS: CADTH claims the literature supports a societal benefit, although admittedly unequal and uncertain. The 2001 Griffin study that purportedly showed that for every $1 spent on fluoridation $38 is saved on dental care costs is cited.
The 2015 paper by Ko/Thiessen that showed Griffin 1) vastly underestimated labour costs ($7 – $8 an hour for professional water managers!) and 2) totally ignored the costs of dental fluorosis repairs which would completely wipe out any savings from water fluoridation, is not included.
Since dental fluorosis has gotten so much worse since Ko/Thiessen’s paper, its increased repair costs would now make water fluoridation a net loser on that alone, not to even mention other health harm costs, such as lowered IQ.
ENVIRONMENTAL: CADTH notes science gaps, quantifies evidence of harm in vague terms, and notes a need for continuous monitoring due to fluoride’s cumulative  nature, “the repercussions of the continual addition of fluoride to community water on ecological receptors in the long term are unknown“.
nature, “the repercussions of the continual addition of fluoride to community water on ecological receptors in the long term are unknown“.
On the uncertainties of fluoride in food chain biomagnification: “Fluoride is one of the main ions responsible for solubilizing beryllium, aluminum, scandium, niobium, tantalum, iron, and tin in natural waters; therefore, there are uncertainties associated with the interactive or synergistic effects of fluoride… the repercussions of the continual addition of fluoride to community water on ecological receptors in the long term are unknown.”
IMPLEMENTATION: Complex, with lots of stakeholders whose input need be weighted.
ETHICS: “This HTA’s scope was to evaluate CWF, and not to systematically examine other oral health interventions, so it is not possible to compare CWF with other oral health using an ethics lens. This means that it is not possible to examine with certainty whether CWF is strictly necessary (i.e.,that there isn’t an alternative that would be equally effective) or whether CWF entails the least restrictive approach to attain its goals.
..CWF has been ethically controversial since its early implementation in the mid-20thcentury…
..The ethics analysis works within the evidence gathered by experts who have developed other domains of this HTA. With this approach, it is taken to be true that CWF does improve oral health (see the Review of Dental Caries and Other Health Outcomes for more detail) and that it ultimately results in reduced financial burden…
Even though there are strong ethical arguments in favour of CWF, it will remain ethically controversial because it is provided without the direct consent of those who receive the intervention. In the case of CWF, this can be ethically justified because the balance of its public health benefits outweigh its measured harms, and are significant enough to override the concerns related to individual choice. ”
SOCIAL DIMENSIONS: This report, mentioned in CADTH’s HTA Protocol, is currently “missing” from CADTH’s HTA web page, without explanation. They have stated via email:
For a number of reasons, CADTH decided not to complete that component of the HTA report. However, we are confident that relevant issues are covered through the ethics analysis and implementation reviews that are also part of the full HTA.
Thank you & Merci,
Stephanie Gabrielle, Central Intake, 613 226 2553 ext. 1221, CADTH
Update, June 15, 2019:
The latest WF ‘summary’ to appear on CADTH’s website:
Therefore- that CADTH statement that fluoridation benefits adults is completely fabricated.
Where did optimum of 0.7 ppm come from in Canada?
It came from the biased Health Canada review (which used Levy and Kumar as external experts…both fluoridation promoters). The so-called “optimum” was based on ONLY two studies. And even one study (Heller, 1999) was incorrectly interpreted.
There are several studies where 0.35 is considered the optimum.
But of course Canada would not want to annoy the Americans (especially Dr. J. Kumar and Dr. S. Levy) or the EPA which eventually, after collusion with the US Dept HHS picked 0.7 ppm as an end point- even though Levy’s group published the finding that determining an optimum was problematic.
So we now have a situation where all of Public Health in North America has no idea if 0.7 ppm is still effective.
Calgary often reaches 0.4 ppm naturally (glacial runoff that feeds the reservoirs- there is tremendous variation in natural fluoride).
CADTH Quote:
Several studies showed fluoridation increases risk of hip fractures (reviewed by the York reviewers). The Toronto vs Montreal study, which produced fluoride measurements in Toronto bone (but not Montreal) that would put someone at risk for hip fracture, was not mentioned.
Elise Bassin’s study (showing increased risk of fluoridation for bone cancer) was not mentioned, neither was the entire 2006 NRC report.
Serious omissions.
CADTH Quote:
“For Down syndrome, IQ, and cognitive function, there was limited evidence that these outcomes are not associated with CWF at the current Canadian levels.“
“For the remaining 16 potential non-dental outcomes, which included death, heart attack, and other conditions, there was insufficient evidence — few studies and of poor quality, or mixed results — to determine if there is an association between CWF and these outcomes.”
Hmm. So, in summary, there was the same level of evidence for benefit as harm i.e. INSUFFICIENT!!!
Why then is there even a cost benefit analysis with cost savings calculated up to 9 significant figures. Really? A high school student knows you can’t get that kind of accuracy starting from a guess.
Assuming some kind of benefit is real (still yet to be quantified!) then why not include cost estimates for harm (fluorosis, bone, arthritis, IQ, ADHD, thyroid, pineal etc etc)???
The conclusions in the other parts of the overall report follow from these flawed premises and false assumptions.